Improving Critical Illness Recovery in the ICU and Beyond
When a woman in her early 30s suffered cardiac arrest due to a pulmonary embolism just days after giving birth to twins, she was transferred to The Johns Hopkins Hospital and placed on life support in the medical intensive care unit (MICU). After eight days on life support and 25 days in the hospital, she began a long journey toward recovery.
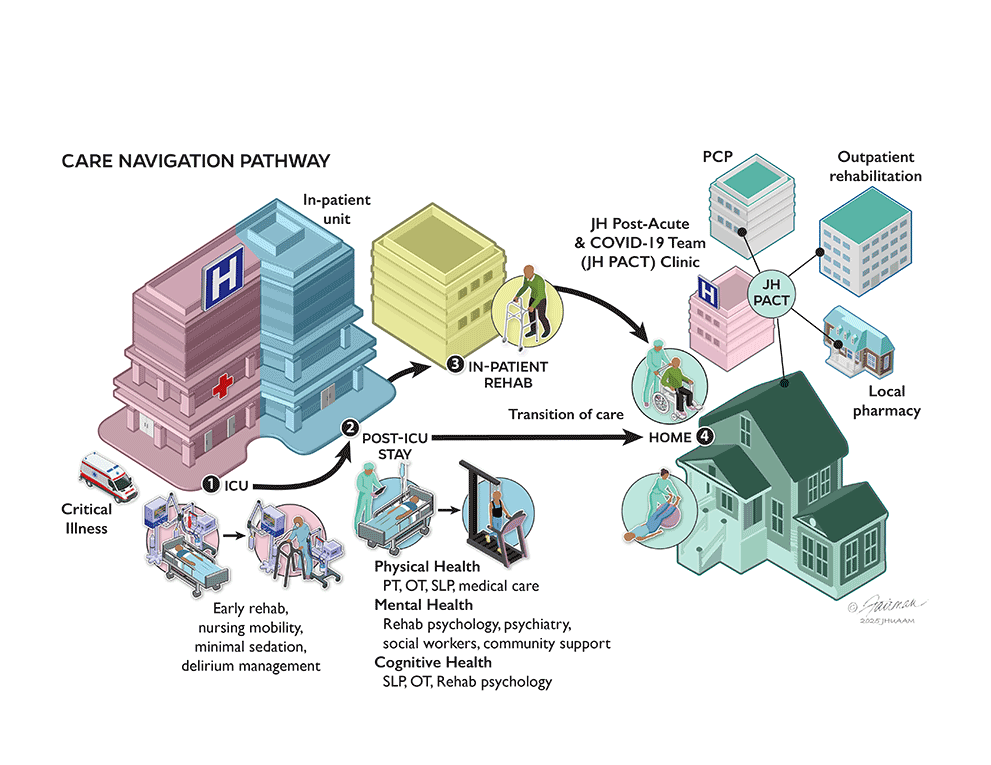
Through Johns Hopkins’ early rehabilitation program in the MICU and the coordinated efforts of the Johns Hopkins Post-Acute and COVID-19 Team (JH PACT) clinic, the new mother regained her independence. The JH PACT team helped manage her follow-up care, including removal of an inferior vena cava filter, medication management and rehabilitation psychology for coping with physical, mental health and cognitive challenges after critical illness. Her story represents the growing community of ICU survivors whose recovery extends far beyond their hospitalization.
Redefining Recovery After Critical Illness
 Dale Needham
Dale NeedhamSurvival is only the first step in critical illness recovery. For many critically ill patients, their days spent in the ICU lead to months or years of lasting complications. These complications, known as post-intensive care syndrome (PICS), leave survivors struggling with muscle weakness, cognitive problems and even post-traumatic stress disorder. These consequences ripple far beyond hospital walls, affecting families, workplaces and communities.
At Johns Hopkins Medicine, research and clinical innovation are reshaping what recovery looks like. In the Outcomes After Critical Illness and Surgery (OACIS) research group, critical care medicine specialists Dale Needham and Ann Parker are leading efforts to understand and reduce the long-term effects of critical illness. Needham served on the Society of Critical Care Medicine task force that coined the term PICS, bringing global awareness to the lasting challenges patients face after ICU discharge. Parker’s research has expanded that understanding, focusing on the emotional and psychological toll of critical illness and identifying strategies to improve patient well-being after hospitalization.
Together, they are advancing multiple groundbreaking initiatives. The NEXIS randomized trial, co-led by Needham, is testing whether combining exercise and nutrition can improve strength and physical function for critically ill patients. Parker, who co-created JH PACT during the pandemic, directs the federally funded Supporting Patients Recovering from COVID-19 (SPaRC) program, which builds on the JH PACT clinic’s foundation to support patients living with long COVID and those recovering from severe critical illness.
 Ann Parker
Ann ParkerJohns Hopkins is also a key site in the National Institutes of Health ARDS, Pneumonia, and Sepsis Consortium, where Needham co-chairs the long-term outcomes subcommittee. This national collaboration is helping connect biological mechanisms with the lived experience of recovery, with the aim of helping laboratory discoveries translate directly into patient care.
Innovation at the Bedside and Beyond
Nearly two decades ago, Needham and The Johns Hopkins Hospital’s MICU pioneered a new standard of clinical care that begins at the bedside. By avoiding unnecessary sedation and encouraging patient mobility, even when on mechanical ventilators, multidisciplinary teams collaborate to protect the brain, nerves and muscles from the harm of sedation and prolonged bed rest. Nurses, physicians, rehabilitation specialists and psychologists collaborate to ensure that survival does not come with the legacy of long-term disability. This practice has become a global model for ICU rehabilitation and has been featured on the front page of the New York Times.
Kelly Johnson, who spent 36 days in the MICU with sepsis and multi-organ failure, described her experience in an article in The BMJ:
“…the early intervention and the progressive mobility approach you discuss was very successful for me, especially combined with occupational therapy. Specifically, occupational therapy focused on fine motor skills (opening bottles, caps, etc.), which was as important as physical therapy addressing the weakness of major muscle groups.”
Early rehabilitation in the ICU is only a starting point in the recovery journey. Recognizing the need for long-term support, Johns Hopkins established the JH PACT clinic, led by Parker. Today, the clinic provides comprehensive care for a broad range of ICU survivors. By integrating pulmonologists, rehabilitation specialists, psychologists, psychiatrists, pharmacists, community health and social workers, the JH PACT clinic comprehensively addresses the spectrum of PICS. Patients are screened for physical, cognitive and psychological impairments, and families are supported with guidance on navigating insurance, work accommodations and community resources. For many, this program has been the bridge from crisis to meaningful recovery.
Expanding Knowledge, Inspiring Hope
The influence of Johns Hopkins extends far beyond Baltimore. For almost 15 years, Needham, along with Parker, have organized the annual Johns Hopkins Critical Care Rehabilitation Conference. This conference brings together a multidisciplinary team of clinicians to present the latest updates to advance best practices in ICU and post-ICU clinical care to attendees from around the world. Moreover, Needham is actively shaping international guidelines, including the ongoing SCCM PICS Clinical Practice Guideline (CPG), the Lancet Neurology Commission on Neurorehabilitation for PICS and the American Thoracic Society/European Respiratory Society critical care rehabilitation CPG. Through the OACIS research group, Johns Hopkins continues to generate evidence that defines the standard of care for recovery in the ICU and beyond.
This leadership is only possible through a unique combination of research, education, clinical innovation and philanthropy. Federal grants provide a foundation, but philanthropy is essential to expand access, sustain programs and accelerate innovation. Unlike cancer or heart disease, the needs of ICU survivors are harder to define and fund. Yet the need is no less urgent. Every gift strengthens our ability to deliver care that restores health, along with independence and dignity.
At Johns Hopkins, we believe survival from critical illness is not enough. With your support, we can continue to transform what it means to recover after critical illness, offering patients and families the hope of life and the promise of living it fully.
For Clinicians Clinical Connection
Clinicians, discover the latest in research and clinical innovation from Johns Hopkins experts. Access educational videos, articles, CME courses and other resources from our world-renowned institution.